Knee Ligament Laxity vs. Torn Ligaments: Interventional Orthobiologics vs. Surgery
There’s an interesting duality between the understanding that loose ligaments should be treated with orthobiologics and the old-school orthopedic surgery approach that only completely torn ligaments are important and can be operated on. This was recently thrust into my consciousness by a sports medicine physician with whom I shared a patient who doggedly claimed that…read more

There’s an interesting duality between the understanding that loose ligaments should be treated with orthobiologics and the old-school orthopedic surgery approach that only completely torn ligaments are important and can be operated on. This was recently thrust into my consciousness by a sports medicine physician with whom I shared a patient who doggedly claimed that this patient had “intact” ligaments that didn’t need to be treated. Let’s explore this important issue this morning.
The Controversy
For decades, a mainstay of orthopedic surgery has been ACL reconstruction. In that world, the ACL is either torn/damaged enough to need replacement, or the patient needs physical therapy. There is often no or little middle ground. However, we know that, like any ligament, the ACL can also be lax. Loose ligaments lead to joint instability, which can cause degenerative joint disease. Hence, with the advent of orthobiologics, determining if an ACL is loose becomes essential. Targeting a lax ACL for treatment is also important.
Many orthopedic practices have begun to add simple orthobiologics, and some have begun hiring non-surgical sports medicine physicians to take over that part of the practice. Recently, I came across a sports med doctor who, IMHO, viewed a patient’s ACL with a surgical binary lens like an orthopedic surgeon. In other words, since the MRI was read as normal and since his more surgically focused exam didn’t show a blown ACL, the patient’s ACL shouldn’t be treated.
This morning, I would like to dive into the controversy as we have two points of view. One states that we need to expand our physical exam skills once we add orthobiologics and identify and treat all lax ligaments that could be causing joint degenerative changes, and the other uses the surgical paradigm that an ACL that looks “intact” shouldn’t be treated.
The Patient
A woman I have known for years was upping her workout game last year when her knee began to hurt. A careful history revealed that when she was younger, a several thousand-pound horse fell on that knee, and while it seemed to heal up since then, that knee was never perfect and always felt “loose.” Her MRI showed moderate cartilage loss under her kneecap and a degenerative lateral meniscus tear. Her exam in my hands showed ACL/ALL, MCL, and LCL laxity, so the treatment plan was clear that we would use PRP intra-articular (IA) and into these lax ligaments. As the treatment unfolded, a sports medicine physician embedded in a local orthopedic surgery group she had also seen was adamant that her “ACL was intact” based on his exam and her knee MRI. He also wanted to inject PRP IA but asserted that she didn’t need ligament injections.
The Traditional Orthopedic Surgery Approach
The good news was that both the sports med doctor and myself agreed that meniscus surgery in a 60+-year-old woman was a non-starter. However, I feel largely because of differences in training and practice environment, the sports med doctor didn’t understand that with orthobiologics, the goal should be to look for mild ligament laxity and, if found, restore knee stability back to or as close to normal as possible. Given that this speaks to a much larger issue that IMHO prevents PRP from reaching its full societal benefit for patients, I thought it was worth a blog.
Ligament Laxity (sub-failure) vs. Ligament Rupture
Let’s face it: orthopedic surgery has focused on ACL injuries that require surgical reconstruction. These are large tears where the ligament is usually completely torn and retracted and is non-functional, causing severe knee instability. However, other types of ligament injuries exist as well.
Ligament injuries are graded 1-3 (1). Grade 1 is damage to the fibers (micotears that can result in laxity), grade 2 is partial tearing, and grade 3 is a complete ligament rupture. I diagnosed this patient with a grade 1-2 ACL injury in addition to knee osteoarthritis. That means that she could have anything from microtearing of her ACL to a partial occult tear.
In my opinion, one of the things that the sports medicine doctor fixated on was the normal MRI read of her ACL. So let’s look at the accuracy of MRI in detecting an ACL rupture (grade 3, a more severe injury than the one discussed here-see the discussion below on sub-failure instability) (7). For those more severe injuries:
“MRI findings for the ACL yielded 60 true-positives (were confirmed on arthroscopy) and 25 true-negatives (without evidence of ACL) with 5 false positive (were miss interpreted to have ACL) and 13 false negative (were not diagnosed clinically) (Table 2; Figure 3), which resulted in 83% sensitivity, 88.37% specificity…”
Again, if this discussion was over a much more severe grade 3 ACL rupture, with a 75% negative predictive value (which means that 1 in 4 ACL ruptures would go undetected by MRI-normal MRI read, but ACL rupture later detected), the idea that a knee MRI can infallibly diagnose a larger ACL tear is ridiculous.
What the sports medicine doctor seemed to miss in this patient, or at least was hesitant to entertain, is the concept of ligament laxity. The idea of sub-failure instability (that a ligament can be damaged to the extent that it doesn’t fail or rupture) is not new and dates back to at least the 1980s (4). This means that the shape of the stress-strain curve is changed, but the ligament remains intact. Let’s explore this idea.
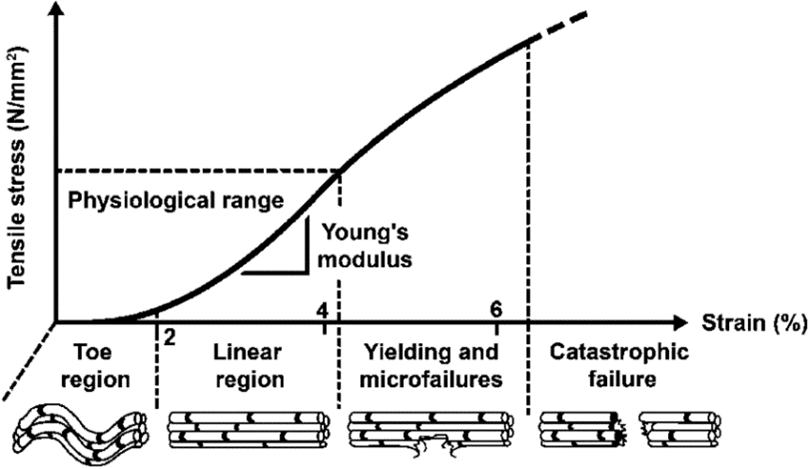
Above is a diagram from a paper on the ACL ligament and tissue engineering (5). Note that if a ligament is stressed in its linear region, it can snap back and live to fight another day. However, if a ligament is stressed into the yielding and microfailure region, it undergoes microinjury. In that case, it can either heal itself or remain lax (grade 1-2 tear) with an altered stress-strain curve. Finally, a ligament can be loaded to catastrophic failure, which would be a complete rupture (grade 3).
As already discussed, orthopedic surgery to date has largely focused on ligaments that rupture. In fact, clinical exam tests like Lachman’s are focused on detecting that ligament state. IMHO, this is the paradigm that sports medicine doctor was using. This patient’s ACL was either so lax that it needed to be replaced, or it was normal, not considering the middle option of loose enough to cause her knee degenerative disease. In other words, the patient’s knee had been subtly unstable since the horse incident, and decades of use and micro-instability had chewed up the cartilage and meniscus in that joint.
Diagnosing Ligament Laxity is Still an Art
In modern medicine, we have severely de-emphasized the art of physical exam. That began with the advent of MRI and was pushed further out the door when managed care caused physicians to see more and more patients on any given clinic day. In this patient, her laxity could be found by looking at the rotational stability of the tibia side to side, as the ACL double-bundle morphology provides that type of stability. In her Lachman’s test, she had a “soft end feel,” meaning that one side gave more at its end range than the other. However, detecting this type of physical exam finding takes years of experience to master.
Detecting ACL laxity due to a grade 1 or 2 tear on MRI or physical exam is difficult (8):
“Clinical examination remains one of the most important steps when evaluating the injured knee. Ligamentous laxity is difficult to quantify and is currently graded subjectively by the examiner (Noyes et al. 1991; Kuroda et al. 2012). Hole et al. found that clinical evaluation is unreliable in the differentiation of a 75 % sectioned ligament from a completely sectioned ligament (Holeet al. 1996).”
Chronic, partial grade 1-2 ACL tears, like the one found in this patient, are notoriously difficult to diagnose (9):
“A partial ACL tear can be observed in 10%–27% of isolated knee injuries.[3] Most patients are unable to comprehend the true nature of their knee morbidity as partial tears lack typical instability, presenting only with quadriceps atrophy on general examination and failure to return to do sports activities. No clinical test is sensitive enough to accurately diagnose a partial ACL tear. Various clinical tests have been advised, but all lack good sensitivity to fathom final diagnosis. The combination of more than one clinical examination helps in the identification of the bundle involved.”
“A partial ACL tear, however, is challenging to identify confidently on imaging.”
Again, the idea that two physicians with different training on this topic could get two different opinions on knee ligament laxity is very real.
Lachman’s Test and MRI
A Lachman’s test was used by the sports med doctor on this patient and is used to detect a grade 3 ACL rupture (which this patient did not have), so it would be the wrong test to look for this type of laxity in the ACL. However, even in that binary world (ruptured or not ruptured), the test, when used during a routine clinical exam, is no better than 50/50 with an average inter-rater reliability of 0.51 (0.15-0.87) (2). That means that 100 physicians could perform this test looking for an ACL rupture, and their assessments would agree no more than half the time. Even instruments designed to look for ACL laxity have high inter-rater reliability and only work reliability in studies when used by the same individual (higher intra-rater reliability) (3). Given that almost all of the physical exam tests that we use in daily practice have at best, moderate inter-rater reliability, you can see why physicians often disagree with what’s found on the physical exam.
Training Your Hands
When I first came out of residency, I was introduced to a local physical therapist, a manual medicine master. He had learned much of what he knew from old osteopaths well-versed in the art of physical exam. Back then, most students in osteopathic medical school were more interested in learning the latest and greatest allopathic medicine, so these osteopathic instructors often found that their DO students were turning up their noses to learning hands-on physical exam skills. In this PT, these old osteopaths found a willing vessel to teach and pass on these advanced manual skills. I was also willing to be trained as I thought it was all fascinating. As I began to take manual physical therapy courses with this PT, I went from being completely unable to use my MD-trained hands to detect things like instability to starting to understand that this was possible. It wasn’t until hundreds of patients and several years later that I became confident in finding unstable joints. In other words, without extensive specialized training, I would have never been able to detect this patient’s knee instability.
PRP Injections
Both the sports medicine doctor and I offered this patient a platelet-rich plasma (PRP) injection. The difference is that I began using PRP in 2005 when this physician was still an undergrad. The practical difference is that I have had almost two decades to observe where PRP is effective and where it fails. The sports med doctor is a recent adopter of PRP.
Every year I perform an analysis of the published PRP RCT literature. The latest 2024 edition shows 144 RCTs with 87% showing superiority or non-inferiority to the comparator. Each circle on this infographic represents an individual RCT
The clinical areas where PRP now has clinical RCT support include:
- Knee OA
- Knee meniscus tear
- Hand OA and other conditions
- Carpal tunnel syndrome
- Hip OA
- Hip tendinopathy
- Shoulder OA, tendinopathy, and rotator cuff tear
- Epicondylitis
- Lumbar radiculopathy, facet syndrome, and DDD
- SI joint pain
- Achilles tendinopathy and partial tears
- Ankle OA
- Plantar fasciitis
In other words, based on the existing RCT data, PRP has been shown to be effective for use throughout the musculoskeletal system for a wide variety of diagnoses.
Focusing on partial tear ACL injuries, the following has been published on using PRP when injected into the joint (NOT into the ACL):
- A successful retrospective observational study in 72 athletes with an 83% return to sports rate (no direct injection into the ACL, only intra-articular) (10).
- A failed RCT in young athletes (no direct injection into the ACL, only intra-articular) (11).
The two opposing clinical outcomes in these studies make sense, as the ACL is surrounded by a sheath (also called a synovial invagination) (16). This means that injecting PRP intra-articular makes little common sense. Why? The PRP won’t be in direct contact with the ligament in a partial ACL tear.
This is what is published on direct injection of PRP into the ligament:
- A case study showing MRI evidence of healing (12).
- A case study of a mucoid ACL showing MRI evidence of healing (14).
- A case series of 19 patients showing normalization of KT-1000 measured laxity in all treated cases with an 82% return to sports rate (13).
- A case series of 42 patients showed a success rate of 90%, showing an objective reduction in laxity as measured by device and a 71% return to sport rate (15).
Hence, the current literature suggests that direct injection into the ACL would be one way to treat this problem. This is using a 25-gauge needle to inject PRP into the ligament once the placement has been confirmed on fluoroscopy. Back in 2015, I developed a direct injection technique into the ACL using fluoroscopic guidance. I have published three studies on selected partial and complete non-retracted ACL tears using orthobiologics and this technique (16-18). One of these is a mid-term analysis of an RCT with that data collection now complete and the final RCT being submitted for publication this month. That RCT data shows MRI evidence of healing of most of these ACLs with a precise injection of bone marrow concentrate plus PRP with high return to sport and low retear rates (about half of those reported for ACL surgery). This final RCT data should soon be published.
Training Physicians in These Techniques
In 2015, I founded a non-profit physician professional organization called the Interventional Orthobiologics Foundation. This organization was funded through a generous multi-million dollar grant from local billionaire John Malone. That group is dedicated to teaching physicians like this sports medicine doctor concepts like how to identify a mildly lax ligament on exam or how to inject an ACL ligament that has micro or a partial tear with PRP or other orthobiologics.
That curriculum I created, and that IOF has now updated, has trained 603 physicians, including dozens from academic medical centers, including Mayo Clinic, Stanford, U Penn, Yale, Vanderbilt, Emory, University of Michigan, University of Miami, University of Wisconsin, UCLA, UC Davis, Baylor, LSU, and the University of Colorado. This same concept is also now taught in courses given by many other organizations.
The upshot? If orthobiologics are going to recognize their full societal impact, physicians using them need to learn new skills. One of those is to stop calling ligaments “intact” based on an MRI report and a quick exam. IMHO, learning to identify lax ligaments and how to treat these areas will improve orthobiologic treatment outcomes. However, that can only happen if physicians who use orthobiologics are open to the idea that we must update the binary orthopedic surgical paradigm that sees ligaments as “ruptured” or “fine.”
_________________________________________________________________________________
- Evans J, Mabrouk A, Nielson Jl. Anterior Cruciate Ligament Knee Injury. [Updated 2023 Nov 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499848/
- Peeler J, Leiter J, MacDonald P. Accuracy and reliability of anterior cruciate ligament clinical examination in a multidisciplinary sports medicine setting. Clin J Sport Med. 2010 Mar;20(2):80-5. doi: 10.1097/JSM.0b013e3181ceca45. PMID: 20215888.
- Runer A, Roberti di Sarsina T, Starke V, Iltchev A, Felmet G, Braun S, Fink C, Csapo R. The evaluation of Rolimeter, KLT, KiRA and KT-1000 arthrometer in healthy individuals shows acceptable intra-rater but poor inter-rater reliability in the measurement of anterior tibial knee translation. Knee Surg Sports Traumatol Arthrosc. 2021 Aug;29(8):2717-2726. doi: 10.1007/s00167-021-06540-9. Epub 2021 Mar 31. Erratum in: Knee Surg Sports Traumatol Arthrosc. 2022 Aug;30(8):2879. doi: 10.1007/s00167-021-06726-1. PMID: 33791824; PMCID: PMC8298217.
- Provenzano PP, Heisey D, Hayashi K, Lakes R, Vanderby R Jr. Subfailure damage in ligament: a structural and cellular evaluation. J Appl Physiol (1985). 2002 Jan;92(1):362-71. doi: 10.1152/jappl.2002.92.1.362. PMID: 11744679.
- Runer A, Roberti di Sarsina T, Starke V, Iltchev A, Felmet G, Braun S, Fink C, Csapo R. The evaluation of Rolimeter, KLT, KiRA and KT-1000 arthrometer in healthy individuals shows acceptable intra-rater but poor inter-rater reliability in the measurement of anterior tibial knee translation. Knee Surg Sports Traumatol Arthrosc. 2021 Aug;29(8):2717-2726. doi: 10.1007/s00167-021-06540-9. Epub 2021 Mar 31. Erratum in: Knee Surg Sports Traumatol Arthrosc. 2022 Aug;30(8):2879. doi: 10.1007/s00167-021-06726-1. PMID: 33791824; PMCID: PMC8298217.
- Nau, Thomas & Teuschl-Woller, Andreas. (2020). Ligament Tissue Engineering: The Anterior Cruciate Ligament. 10.1007/978-3-030-18512-1_7-1.
- Kostov H, Stojmenski S, Kostova E. Reliability Assessment of Arthroscopic Findings Versus MRI in ACL Injuries of the Knee. Acta Inform Med. 2014 Apr;22(2):111-4. doi: 10.5455/aim.2014.22.111-114. PMID: 24825936; PMCID: PMC4008041.
- Ohashi, Bruno & Ward, James & Araujo, Paulo & Kfuri Jr, Mauricio & Pereira, Hélder & Espregueira-Mendes, Joao & Musahl, Volker. (2015). Partial Anterior Cruciate Ligament Ruptures: Knee Laxity Measurements and Pivot Shift. 10.1007/978-3-642-36569-0_85.
- Chandra, Abhishek; Agarwal, Aakanksha1,; Azam, Md. Quamar. Demystifying Partial Tears of the Anterior Cruciate Ligament: A Review of Current Diagnostic and Management Strategies. Journal of Arthroscopy and Joint Surgery 10(1):p 1-9, Jan–Mar 2023. | DOI: 10.4103/jajs.jajs_126_22
- Herdea A, Struta A, Derihaci RP, Ulici A, Costache A, Furtunescu F, Toma A, Charkaoui A. Efficiency of platelet-rich plasma therapy for healing sports injuries in young athletes. Exp Ther Med. 2022 Mar;23(3):215. doi: 10.3892/etm.2022.11139. Epub 2022 Jan 11. PMID: 35126718; PMCID: PMC8796279.
- Zicaro JP, Garcia-Mansilla I, Zuain A, Yacuzzi C, Costa-Paz M. Has platelet-rich plasma any role in partial tears of the anterior cruciate ligament? Prospective comparative study. World J Orthop. 2021 Jun 18;12(6):423-432. doi: 10.5312/wjo.v12.i6.423. PMID: 34189080; PMCID: PMC8223727.
- You CK, Chou CL, Wu WT, Hsu YC. Nonoperative Choice of Anterior Cruciate Ligament Partial Tear: Ultrasound-Guided Platelet-Rich Plasma Injection. J Med Ultrasound. 2019 Apr 10;27(3):148-150. doi: 10.4103/JMU.JMU_121_18. PMID: 31867179; PMCID: PMC6905270.
- Seijas R, Ares O, Cuscó X, Alvarez P, Steinbacher G, Cugat R. Partial anterior cruciate ligament tears treated with intraligamentary plasma rich in growth factors. World J Orthop. 2014 Jul 18;5(3):373-8. doi: 10.5312/wjo.v5.i3.373. PMID: 25035842; PMCID: PMC4095032.
- Seeto AH, Wilson MD, McMeniman M, Astori IP. Severe mucoid degeneration of the anterior cruciate ligament (ACL) treated with conservative arthroscopic debridement and platelet-rich plasma (PRP) injection. BMJ Case Rep. 2024 Feb 13;17(2):e257217. doi: 10.1136/bcr-2023-257217. PMID: 38350698; PMCID: PMC10868321.
- Koch M, Mayr F, Achenbach L, Krutsch W, Lang S, Hilber F, Weber J, Pfeifer CG, Woehl R, Eichhorn J, Zellner J, Nerlich M, Angele P. Partial Anterior Cruciate Ligament Ruptures: Advantages by Intraligament Autologous Conditioned Plasma Injection and Healing Response Technique-Midterm Outcome Evaluation. Biomed Res Int. 2018 Jul 25;2018:3204869. doi: 10.1155/2018/3204869. PMID: 30148163; PMCID: PMC6083554.
- Duthon VB, Barea C, Abrassart S, Fasel JH, Fritschy D, Ménétrey J. Anatomy of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):204-13. doi: 10.1007/s00167-005-0679-9. Epub 2005 Oct 19. PMID: 16235056.
- Centeno C, Lucas M, Stemoer I, Dodson E. IMAGE-GUIDED INJECTION OF ANTERIOR CRUCIATE LIGAMENT TEARS WITH AUTOLOGOUS BONE MARROW CONCENTRATE AND PLATELETS: MIDTERM ANALYSIS FROM A RANDOMIZED CONTROLLED TRIAL. Bio Ortho J Vol 3(1):e29–e39; October 5, 2021.
- Centeno C, Markle J, Dodson E, Stemper I, Williams C, Hyzy M, Ichim T, Freeman M. Symptomatic anterior cruciate ligament tears treated with percutaneous injection of autologous bone marrow concentrate and platelet products: a non-controlled registry study. J Transl Med. 2018 Sep 3;16(1):246. doi: 10.1186/s12967-018-1623-3. PMID: 30176875; PMCID: PMC6122476.
- Centeno CJ, Pitts J, Al-Sayegh H, Freeman MD. Anterior cruciate ligament tears treated with percutaneous injection of autologous bone marrow nucleated cells: a case series. J Pain Res. 2015 Jul 31;8:437-47. doi: 10.2147/JPR.S86244. PMID: 26261424; PMCID: PMC4527573.
- Moseley JB, O’Malley K, Petersen NJ, Menke TJ, Brody BA, Kuykendall DH, Hollingsworth JC, Ashton CM, Wray NP. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2002 Jul 11;347(2):81-8. doi: 10.1056/NEJMoa013259. PMID: 12110735.